|
|

Kérdezz-felelek
Lenne 1-2 konkrét kérdésem. /SOS hajhullás/
Az én esetemben tehát, hajhullásra nem tanácsos olyan vitamin készítményt sem szedni, ami egyéb vitaminokon kívül jódot is tartalmaz? A Béres-cseppben nincs jód, de mivel az immunrendszer működését támogatja nincs befolyása akkor, ha autoimmun betegség lehet?
Az előbbiekben leírt laborleletek adnak gyanút csökkent működésű pajzsmirigyre v. gyulladásra?
És szeretném még megkérdezni, h. a hormonszintjeim megfelelőek-e, mert a referencia tartományt nem tüntették fel. /
Még egyszer KÖSZÖNÖM!
a bÉRES CSEPPET SZEDHETI.
jÓ GÉSZSÉGET KÍVÁNOK:
Tisztel Professzor Úr!
Örülök, h. rátaláltam Önre!Személyesen is fel szeretném keresni.
Addig is szeretném a segítségét kérni! SOS! Mert nagyon hullik a hajam.
Tudom, hogy ez nem ilyen egyszerű, de tálán lenne 1-2 javaslata, meglátása, tanácsa, amit előre is köszönök!
A fokozottabb hajhullás 1.5-2 hónapja kezdődött.
Előzmények: -terhesség után /13 éve/ pajzsmirigyben diagnosztizált hideg ill. meleg göb
- azóta túlsúly
- menstr. ciklus problémák /kimaradó menstr./
- utóbbi időben, nem tudom pontosan, talán izületi panaszok /egyik karon könyök, ill egyik lábon
külső talp él v. ujj csont fájdalom, járáskor pattogó hang /
Labor leletek:éhgyomri vércukor: 6,4 Terhelés: 30\' 11,1 60\' 10,7 90\' 9,3 120\' 6,9
koleszterin: 6,8 mmol/l triglicerid: 3,38 mmol/l
CK: 221 E/l
Vvt szám: 4,360 T/l Vas : 18,4 umol/l
Kálcium: 2,34 mmol/l Foszfor: 0,85 mmol/l PTHN1 6,73 pmol/l
TSH: 1,480 mE/l FT4: 13,80 pmol/l FT3: 4.64 pmol/l
Hormonok /a ciklus 5. napján/
- Tesztoszteron: 0,9 nmol/l
- FSH: 6.0 mE/ml LH: 2,9 mE/ml
- Progeszteron: 1,1 nmol/l Prolactin: 390.0 mE/l
- Ösztrad.: 124 pmol/l
- Kortizol :601.0 nmol/l DHEA :6.30 umol/l
Tisztelettel: minden jót kívánok Önnek!
Tisztelt Kérdező!
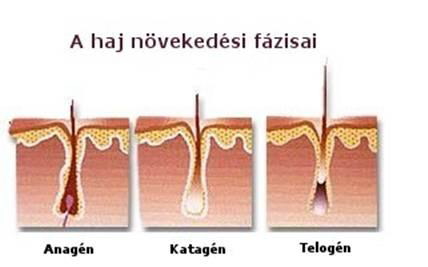
A megtisztelő kérdése valóban összetett. Mielőtt a további részletekbe mennék egy kérésem van, hogy anorganikus jódot az esetleeges javaslat ellenére se szedjen be! A hajhagymák növekedésének három fázisa van. Az első az u.n. „anagén”, ez növekedés gyors fázisa, amely időszakban a haj növekedése 28 naponként akár 1 cm-t is elérhet. Ez az időszak néhány évig is tarthat. Ezt követi az u.n. „katagén” szakasz, amely a gyors növekedés végét jelenti és néhány (2-3 ) hétig tart. Majd a „telogén” fázis köszönt be, amikor a hajhagymák nyugvó állapotba kerültnek. Ez az összes hajszál 10-15%-t is jelentheti és 100-120 napig is eltarthat. Lényeges ez a szakasz is, mert biztosíthatja a kihullott hajszálak utánpótlását. Természetes, hogy fésülködéskor, vagy hajmosáskor több hajat veszítünk, mint egyébként. Normálistól eltérő hajhullásról csak akkor beszélhetünk, ha azt vesszük észre, hogy a korábbinál jobban hullik a hajunk, fénytelenné, töredezetté válik, reggel, ébredés után a párnánkon sok hajszálat találunk, vagy már kisebb fizikai hatás alkalmával is csomókban szakad ki hajunk. Ezekben az esetekben minden alkalommal érdemes kideríteni, hogy milyen okok állnak a háttérben.
A hajhullást számos tényező válthatja ki:
• Hormonok (tesztoszteron szabad tesztoszteron, PCOS,
• Fogamzásgátló
• autoimmun betegség (ez érintheti a hajhagymákat is!)
• Stressz
• mérgező anyagok
• Gyógyszerek
• Sugárkezelés
• táplálkozási rendellenességek
• vitaminhiányok.
A hajhullást számos tényező válthatja ki: hormonok, fogamzásgátló, autoimmun betegségek (pajzsmirigygyulladás), nőkben fokozott férfi hormontermelődése, stressz, mérgező anyagok, gyógyszerek, sugárkezelés, táplálkozási rendellenességek.
A haj növekedésének alapja a hajhagyma, amelynek képződését számos örökletes és hormonális tényező befolyásolja.
A férfi hormonok szintjének emelkedése a vérben és a hormonok iránti érzékenység fokozódása egyaránt lényeges ebben a kérdésben. A férfi hormonok nőkben a petefészekben és a mellékvesékben (ritkán más szervekben) képződnek. A hormonálisan kevésbé aktív férfihormont, a tesztoszteront, a vérben lévő fehérje, az SHBG („Sex Hormone Binding Globulin") juttatja el a szervezet különböző részeibe. Az SHBG-ről lehasadó tesztoszteronból a bőrben különböző mennyiségben jelenlévő 5-alfa-reduktáz enzim egy rendkívül aktív férfihormont, a dihidro-tesztoszteront képezi, amely elsődlegesen bűnös a hirzutizmusért.
Az androgén típusú hajhullásnak több oka lehet:
Döntően a vérben, de főleg a bőrben képződő férfi hormon (FTI) a fontos ebben a kérdésben, de a következőket is ki kell(ne) vizsgálni:
• PCOS (policisztás ovárium tünet együttes)
• Menstruációs hormonális zavarok
• Mellékvesék túlműködése és daganatai
• Kóros elhízás, fokozott inzulin szint
• Petefészek egyes daganatai
• Pajzsmirigy betegségei
A kezelés oki, tehát tisztázni kell a hajhullás okait.
A kezelések támadáspontjai a következők:
• Csökkentik a férfihormonok termelődését és vérszintjét
• Növelik a női hormonok mennyiségét és vérben, ill. a bőrben a szintjét
• Gátolják az 5-alfa-reduktáz enzim működését a bőrben
• Befolyásolják a kisiklott pajzsmirigyműködést
A legújabb kísérleti adatok igazolták, hogy a pajzsmirigy hormonjainak jelentős szerepe van a nők hajának növekedésében. Ezt kísérletekkel bizonyították. Azt vizsgálták, hogy a nőkből kozmetikai műtétek során kivett hajhagymák növekedése hogyan változik pajzsmirigy hormonok hatására. A kivett hajhagymákat tenyésztették és vizsgálták az egyes fázisokat a pajzsmirigy két hormonjának: a trijódtironinnak és a tiroxinnak a jelenlétében. Meglepetésükre azt figyelték meg, hogy ezek a hormonok növelték az anagén fázis hosszúságát, sőt fokozták a bőr pigmentációját is. A kísérlet azért jelentős, mert felhívja a figyelmet arra, hogy a pajzsmirigy hormonjainak hiánya felelős lehet a nők fokozott hajhullásáért, A száraz és ritka haj mellett pajzsmirigyhormon szint csökkenésére utalhatnak az alábbi tünetek: fáradékonyság, a koncentrációs képesség romlása, lelassult anyagcsere, mozgás, beszéd és gondolkodás. Aluszékonyság, hízás, szorulás, fázékonyság lesz jellemző, az arc felpuffad, csökkent a libidó (nem vágy). A bőr hideg, száraz, sápadt és durva. A kezek fájhatnak, a körmök töredeznek, a testen ödémák alakulhatnak ki. A pajzsmirigy gyulladása, ill. csökkent működése jól kezelhető gyógyszerekkel.
Elérhetőségem: 06-30-631-9309
Jó egészséget kívánok, tisztelettel:
Kedves Professzor úr! 2010. januárjában kivizsgált az Irgalmas Kórházban. Semmit nem talált akkor- a PCOS miatt sportot, diétát javasolta. /Akkor Diane 35-t szedtem egy ideje, nem akartam babát még mert nem volt párom/. Most férjhez mentem családot alapítanánk szívesen, de a Diane után jöttek az andorgén tüntetek erősen és a rendszertelen menzesz is. Az ultrahang is mutatja a sok kis cisztát. Clomifen kezelés volt 2 ciklusban-nem reagálok rá. Hormonvizsgálat volt, tesztoszteron kicsit magas, FS/LH arány megborult. A éhhomi cukor 5 alatti , a terhelt cukor szintén 5 alatt. Nem akartak Metformit adni,hogy jó a cukrom. Kértem, a nőngyógyásztól külön egy inzulinos vizsgálatot is.Most csináltattam inzulint is végre. A 120 perces eredménye 21 körüli volt.Mit javasolna?Várom válaszát amit előre is köszönök. Üdv, Tímea
Kedves Timea!
Örülök, hogy babát szeretne és ennek biztos nem lesz akadálya. A Diane35 mellett valóban nem lett volna célszerű más kezelést elkezdeni. A kezelés elkezdése előtt néhány kiegészítő vizsgálatra is volna szükség (gondolom a nőgyőgyász erről felvilágosítást adott). Ezek birtokában lelehtne elkezdnei a további kezelést. Ugyanis a PCOS jelentése policisztás (sokhólyagú) ovárium szindróma . Bár az elnevezés csupán a petefészek (ovarium) betegségére utal, mégis számos hormonális és anyagcsere eltérés is áll hátterében, melyek szerteágazó tüneteket produkálnak. A hormonrendszerben keletkező zavar jellemzően nem egyik pillanatról a másikra jelentkezik, a tünetek a legtöbbször hosszú időn át, folyamatosan alakulnak ki. Egyéntől függően előfordulhat az is, hogy nem az összes, csak egy-két tünet jelentkezik.
A PCOS tünetei:
• Rendszertelen vagy hiányzó peteérés és menzesz
• Meddőség
• Sok, apró ciszta a petefészekben
• Aknés, pattanásos bőr
• Emelkedett inzulinszint a vérben, inzulinrezisztencia vagy lappangó diabétesz
• Kifejezett férfias szőrzet az arcon hason, végtagokon („hirsutizmus”)
• Hajhullás, esetleg férfias jellegű kopaszodás
• Súlyproblémák, elhízás
Lényeges, hogy az egyes tényezők összefüggenek és ok-okozati viszonyban is vannak egymással. Ugyanis az elhízás nem csak a PCOS következménye, de egyben kiváltó oka is lehet. Az elhízás gyakran jár együtt a ”metabolikus szindrómának” nevezett kórképpel. A „metabolikus szindróma” jelei a magas koleszterin, megnövekedett vérzsír- és vércukorértékek, magas vérnyomás. Ez is mutatja, hogy a zsírszövet nem egyszerűen energiaraktár, hanem fontos endokrin szerv. Az utóbbi évek kutatásai felhívták figyelmünket arra is, hogy a PCOS-s betegek egy részében a rendelkezésre álló érzékeny ultrahang vizsgálat sem tud cisztát kimutatni. Ez is azt mutatja, hogy a ciszta csak egy kóros folyamat eredménye és nem okozója. A PCOS kialakulásában döntő szerepet játszanak az örökletes tényezők Hallom a figyelmes olvasó kérdését: „amennyiben örökletes ok van a háttérben, akkor miképpen lehetséges, hogy anyámnak nem volt ilyen betegsége nekem pedig igen?„Erre a válasz kettős: egyrészt korábban a betegséget nem vagy alig ismertük. A legfontosabb azonban az, hogy az örökletes háttér inkább a hajlamot jelenti és a környezeti tényezők a meghatározó fontosságúak ahová számos anyag: vegyszerek és mérgező anyagok, hormonszerű rovarirtó szerek, növényi hormonok (u.n. EDC anyagok, erről ezen a honlapon a fuzárium gomba kapcsán az elmúlt évben már írtam) sorolhatók. Az egyértelmű fogalmazás megköveteli, hogy sokféle anyaga lehetséges, sőt azok együttese lehet a felelős, de ma a tudomány nem ismer egyetlen „bűnös anyagot„. A PCOS kialakulása általában már a pubertás előtt megindul, létrejöttében számos bonyolult mechanizmus játszik szerepet, amelynek részletezésébe azért nem kezdek, mert attól tartok, hogy ez a megértést inkább gátolná, mint elősegítené. A lényeg leegyszerűsítve az, hogy hyperandrogén (férfias) típusú hormonális változások jönnek létre.
Mi történt velem? Teszik fel a kérdést a PCOS-ban szenvedők
A hormonrendszerben keletkező zavar jellemzően nem egyik pillanatról a másikra jelentkezik, a tünetek a legtöbbször hosszú időn át (éveken), folyamatosan alakulnak ki. Egyéntől függően előfordulhat az is, hogy nem az összes, csak egy-két tünet jelentkezik.
Melyek a PCOS tünetei?
• Rendszertelen vagy hiányzó peteérés és menzesz
• Meddőség
• Sok, apró ciszta a petefészekben
• Aknés, pattanásos bőr
• Emelkedett inzulinszint a vérben, inzulinrezisztencia vagy lappangó diabétesz
• Férfias jellegű szőrzet az arcon és a testen (hirzutizmus)
• Hajhullás, esetleg férfias jellegű kopaszodás
• Súlyproblémák, elhízás
• Gyakran társul a pajzsmirigy betegségeivel
Fontos megjegyeznünk, hogy az elhízás nem csak a PCOS következménye, de egyben kiváltó oka is lehet. Az elhízás gyakran jár együtt a metabolikus szindrómának nevezett kórképpel. A metabolikus szindróma jelei a magas koleszterin, emelkedett vérzsír- és vércukorértékek. Mindezek együttese, különösen öröklött hajlam esetén nagy mértékben növeli a PCOS kialakulásának kockázatát.
Melyek a legfontosabb lépcsői a PCOS-nak?
• Genetikai, örökletes tényezők (családi adatok ismerete fontos
• Kifejezett inzulin rezisztencia- Ez azt jelenti, hogy az inzulin szint ugyan magas, de hatását nem tudja kifejteni. Ennek sokféle oka van, leggyakoribb a kóros elhízás. Ez egy ördögi kört eredményez. Minél magasabb az inzulin szint, annál nagyobb az étvágy és növekszik a testsúly, romlik a PCOS tünet együttes, majd a további szövődmények: magas vérnyomás, cukorbetegség is felléphet. A magas inzulin szint . csökkenti mind a szex-hormon kötő fehérje (SHBG), mind az inzulinszerű növekedési faktor (IGF) kötő fehérje szintjét, aminek fokozott nemi hormon lesz a következménye. Ez utóbbi fokozza egyrészt a petefészek kóros működését, másrészt viszont szintén növeli a mellékvese „stressz hormon”(kortizol) metabolizmusát. Ez az összetett folyamatok kóros önerősítési köröket hoznak létre, s magyarázzák, hogy a PCOS súlyosbodását sokszor súlygyarapodás idézi elő.
• Megváltozik az agyalapi mirigy hormonjainak (LH, FSH, prolactin) termelődése
• A petefészek fokozott mértékben termel férfi nemi hormonokat
Diagnózis
A PCOS diagnózisa a Rotterdami kritériumok (2003) alapján történik. A diagnózis akkor állapítható meg, ha
két tünet jelen van a következő háromból:
a/ oligo- vagy anovuláció,
b. androgén túlsúly klinikai és/vagy laboratóriumi jelei,
c. ultrahanggal igazolt PCOS és
A beteg vizsgálata
A beteg kikérdezése és vizsgálata alapvető fontosságú (ne előzze meg a hormonális vizsgálatokat!)
Mit célszerű vizsgálni?
• Vizsgálni kell a hirsutismus súlyosságát
• A hajhullás, alopecia mértékét és jellegét
• Más agyalapi betegség (Cushing-kór) jeleit
• Meg kell határozni a testsúlyt, has körfogatot és vérnyomást.
• A hormonvizsgálatok egy részét (az „alapvizsgálatokat”) a ciklus (ha van) első napjaiban (2-4. nap között) kell végezni. Ilyenek LH, FSH, tesztoszteron, SHBG, prolaktin.
• Célszerű a szabad tesztoszteron mérése vagy a szabad tesztoszteron index kiszámítása
• Szükség van a teljes körű lipid vizsgálatra, a szénhidrát anyagcsere időszakos ellenőrzésére (HOMA-IR), azaz az inzulin rezisztencia meghatározására
• A pajzsmirigy diszfunkció kizárása céljából hormonális és immunológiai vizsgálatok célszerűek.
PCOS kezelése
Rendkívül összetett feladat és gyakran eltérő, mivel a kiváltó okok is azok!
A kezelés elvi céljai:
- a hyperandrogen állapot csökkentése,
- a meddőség kezelése,
Jó egészséget kívánok:
A bal lebenyben (51 x 53 x kb. 80 mm) levő eddigi két nagyobb göb egyesült, 58 mm legnagyobb átmérővel s így quasi kitölti a lebenyt. A trachea jobbra dislocalt, comprimalt. Férjem a műtéttől elzárkózik.
Tud-e Professzor Úr biztató véleményt mondani!
Válaszát reménykedve várom. Szívélyes üdvözlettel: Faga-Nagy Mária
Köszönöm, hogy kérdésével megtisztelt. A göbös betegségek kezelése attől függ, hogy a nagyságán túlmenően (amit szépen leírt) milyen felépítésű, van-e gyulladás, mit mutat a citológiai kép. Eygébként a pajzsmirigy göbös betegségei azért is fontosak, mert ide tartoznak a jó és rosszindulatú daganatai is. Ezek egyrészt fokozott működéssel járó göbök lehetnek, amelyek sok hormont termelnek („meleg” göbök). Ezek kimutatásához a pajzsmirigy megtapintása és hormon-meghatározások mellett izotópos vizsgálat is szükséges. A túlműködés a hagyományos gátlószeres kezeléssel csak átmenetileg gyógyítható (!), a készítmény elhagyása után a túlműködés ismét jelentkezik. A végleges gyógyulás izotóp terápiától, esetleg műtéttől várható.
Fontos: ezek nem autoimmun betegségek!
A rosszindulatú daganatok nem járnak túlzott hormon-termeléssel, különböző méretű „hideg” göbök formájában jelentkeznek. A diagnosztizálásukhoz az un. tumor marker (thyreoglobulin) meghatározása és szövettani, citológiai vizsgálat szükséges („vékonytű biopszia”). Kezelésük műtéttel és izotóppal lehetséges.
Jó egészséget kívánok:
Pajzsmirigy alulműködésem van de a t3,t4 értékek mindig a jó tartományban vannak,ez már többszöri labornál is így volt.A TSH mindig 5 és 6 közötti értéket mutat de a t3,t4 mindvégig normál határon belüli.ATPO-t még nem néztek eddig.Ön szerint tanácsos lenne?Ha kiderül,hogy az ATPO jó,akkor mi okozhatja még az alulműködést.A jódhiányról is hallottam még,hogy ez is okozhat alulműködést.
Ön mit tanácsol milyen vizsgálatokat végeztessek,hogy kiderüljön az emelkedett TSH oka?
Nagy valószínüséggel Önnek ún. szubklinikus hypothyreosisa van. Szubklinikus hypothyreosisnak nevezzük azt az állapotot, amikor a szérum TSH-szintje meghaladja a normális felső határt, ugyanakkor a szabad tiroxin (FT4) még a normális értékhatárokon belül van. Válaszra váró kérdés, hogy az úgynevezett normális FT4-szint mellett hogyan jöhet létre emelkedett szérum-TSH-koncentráció. Az egyik legelfogadottabb nézet szerint, egészséges egyén esetében viszonylag szűk határok között ingadozik az egyéni szérum-T4- és trijódtironin- (T3-) szint, ezzel szemben az átlagpopuláción alapuló referenciatartomány határértékei egymástól távol vannak. Amit mi a normális referenciatartományon belüli pajzsmirigyhormon-koncentrációnak nevezünk, lehetséges, hogy az adott egyén esetében már nem normális, amelyre az agyalapi mirigy már reagál. További kérdés, hogy ez az elváltozás már a manifeszt hypothyreosis előhírnökének tekinthető-e, vagy csak kompenzált biokémiai folyamatról van szó. A szubklinikus hypothyreosis diagnózisa attól is függ, hogy a TSH-vizsgálat milyen módszerrel történik, és mit tekintünk a TSH-szint normális felső határának. Gyakoriságát különböző szerzők egymástól eltérően ítélik meg (1,3–17,5%); mindenesetre az megállapítható, hogy főleg nőknél, az életkor előrehaladtával gyakoribbá válik, és gyakorisága függ a jódellátottságtól is. Az esetek 75%-ában a szérum-TSH-szint csak kismértékben emelkedett meg (5–10 mE/l) és az esetek 50–80%-ában thyreoidea-peroxidáz elleni antitestpozitivitást lehet kimutatni . Ennek jelentőségét mutatja, hogy egy 20 éves követési időszak alatt évente, az emelkedett TSH-szintű és pajzsmirigyellenanyag-pozitív nők 4,3%-ánál alakult ki manifeszt hypothyreosis, míg az ellenanyag-negatív esetekben ez az arány 2,6% volt. A szubklinikus hypothyreosis kialakulásában, a manifeszt hypothyreosishoz hasonlóan, endogén és exogén tényezők játszanak szerepet .
További részletes enokrin, ill. immuno-endokrion kivizsgálást javaslok.
Jó egészséget kívánok:
Körülbelül egy éve derült ki, hogy autoimmun pajzsmirigy betegségem van! 26 éves vagyok. Előtte nem volt rá utaló jel, de a nyakamon egyre jobban látszik. Az én pajzsmirigyem nem működik se alul, sem túl. Megcsináltatta az orvosom a nyaki ultrahangot. Ez alapján: diffúzan inhomogén, szétszórt kisebb gócok. Göb nincs. Tehát semmi komoly.
TRAK, TSH negatív. anti TPO-ra még várok. Az lenne a kérdésem, ha az is negatív, akkor merre induljak el? Mert engem nem hagy nyugodni, hogy nem tudom mi okozza!!!!!! Van még egy tünetem! A havi ciklusom idelyén megduzzad a pajzsmirigyem, és olyan rossz a közérzetem! Olvastam, hogy rengeteg oka lehet, de mégis? Mit lehetne még tenni? Gondoltam egy teljes allergia vizsgálatra? Azt érdemes volna csináltatni? Illetve milyen vizsgálatot javasolna még?
Nem tudom elhinni, hogy a pajzsmirigyem jól működik, ellátja feladatát, mégis megnagyobbodott valamitől. Sokat olvastam az autoimmun betegségekről, de akkor nem az okot kellene megkeresni, és azt gyógyítani, minthogy megvárni, míg a pajzsmirigy alul, vagy túl fog működni, esetleg a mérete növekszik??????????
Válaszát előre is köszönöm!!!!!!
Tisztelettel: V.Éva
Jól gondolja, az okokat kell(ene) megkeresni. Egy-egy laboratóriumi vizsgálat olyan mintegy pillanatfelvétel, a folyamatot nem ábrázolja. Az immunrendszer feladata a szervezet saját szöveteinek és sejtjeinek („integritásának”) védelme. Amennyiben ebben hiba támad, akkor az immunrendszer sejtjei és az általuk termelt fehérjék (antitestek) saját szöveteik, „antigénjeik” ellen támadnak és ez a sejtek működésének gátlásához, esetleg a működésük növekedéséhez vezethet. Az autoimmun betegségeknek didaktikai okokból elkülönítjük a szisztémás és az egy-egy szervre lokalizálódó szerv-specifikus formáit. Ezekre a betegségekre jellemző, hogy öröklődnek, főleg nőkben fordulnak elő és gyakran társulnak egymással (pl. pajzsmirigybetegség cukorbetegséggel, meddőséggel stb).. Az autoimmun eredetű szerv-specifikus pajzsmirigybetegségeknek két fő formája ismert: az autoimmun pajzsmirigygyulladás (Hashimoto betegség) és Basedow-Graves kór.
A krónikus autoimmun gyulladás kezdetben gyakran tünetmentes, de együtt járhat átmenti pajzsmirigy érzékenységgel vagy megnagyobbodással, tömött tapintatú strúmával, esetleg hőemelkedéssel. Következményeként tartós alulműködés is előfordulhat már a betegség kezdetén előfordulhat. A pajzsmirigy komponensei: a Tireoglobulin és a pajzsmirigy peroxidáz enzim (TPO) elleni antitest mérése fontos. Észlelésekor a pajzsmirigy vékonytű biopszia (szövettani vizsgálatot) is szükséges lehet. A betegség korai felismerése azért is fontos, mert a tünetmentes forma („szubklinikus”) is jelentős rizikófaktora számos betegségnek. A betegség lefolyásában négy stádiumot különíthetünk el: l Hiperfunkciós stádium: betegség kezdetétől számított 1-6 hét. A tünetek a sejtek károsodása miatt felszabaduló jelentős mennyiségű hormon következtében jönnek létre („destruktív hyperthyreosis”). 2. Hipofunkciós stádium: a betegség kezdetétől számított 8. héttõl 4-6 hónapig. 3. Regenerációs stádium: A betegség kezdetétől számított 7-12 hónap. 4. Definitív stádium: ha a regeneráció teljes, akkor a beteg gyógyult, míg a betegek többségében súlyos, enyhe, esetleg szubklinikus hypothyreosis alakul ki (a TSH szint emelkedett, de a perifériás hormonok szintje az élettani határokon belül van). A hypothyreosis egyes formáinak meghatározásában lényeges az élettani TSH szint definiciója. A szuperszenzitiv TSH (sTSH) módszerek lehetővé tették a szubklinikus és az enyhe hypothyreosis megkülönböztetését. A sTSH 2.5 mU/l felső szintjét (!) az irodalom általában elfogadja, de számos, a szerzők által is leírt megkötést is megfogalmaz. A fiziológiás TSH szint felső határának 4,5-ről 2,5- mU/l-re csökkentése azt is eredményezte, hogy az Egyesült Államokban a szubklinikus hypothyreosisos betegek száma meghaladja a 20 milliót. A TSH meghatározásának fontosságát senki nem vonja kétségbe, de annak abszolutizálása félrevezető lehet. Ezért is lehet támogatni azt a legújabb véleményt, hogy a diagnózis megállapításakor ne csak a TSH értéket, hanem a familiáris adatokat (előfordul-e pajzsmirigybetegség a családban?) az immunológiai tesztek eredményét, spontán abortuszokat, egyes gyógyszerek fogyasztását (anorganikus készítmények:pl. Cordaron, betadin kúp, oldat) is célszerű figyelembe venni. Fontos, hogy még akkor ismerjük fel a betegséget, amikor a gyulladás már fennáll (antitestek magasak!), de még a pajzsmirigy működése nem csökkent (élettani hormonértékek!) . A kezelés szerencsére nem a műtét, hanem a megfelelő, egyénre szabott immun-moduláns gyógyszeres kezelés, esetleg pajzsmirigy hormonpótlás (egyéni mérlegelés alapján). „Ne a laboratóriumi értékeket kezeljük, hanem a beteget”!.
Ráadásul az autoimmun betegségek gyakran társulnak egymással. Eért a pajzsmirigy kezelése előtt mindig legyen kérdés az, hogy:
• Van-e mellékvese betegsége, Addison kórja?
• Van-e más immuneredetű endokrin betegsége (pl. inzulinnal kezelt cukorbetegség, mellékpajzsmirigy gyulladás?)
• Van-e más autoimmun eredetű betegsége:
o Meddőség, menzesz zavarok?
o Gyomor-bélgyulladás, nyelvgyulladás?
o Hajhullás?
o Vészes vérszegénység („anaemia perniciosa”)?
o Ízületi gyulladás?
o Vitiligo (bőrfestékhiány)?
o Van-e ismeretlen eredetű alacsony vérnyomás?
o Van-e fokozott hajlam fertőzésekre?
o Van-e idegrendszeri autoimmun betegsége („myastenia gravis, sclerosis multiplex”)?
o Van-e szívizomgyulladása?
Ezért az egyik tünet vagy betegség felismerése után az okok keresése mellett arra is gondolni kell, hogy más, társuló betegség van-e, esetleg lappangó formában. Tudom, hogy ez a mechanikussá, „ún. protokollokká” alakult orvoslásban gyakran „elsikkad”, pedig erre gondolni valóban nem pénzkérdés!
Jó egészséget kívánok, tisztelettel:
Érdeklődni szeretnék, hogy van-e magánrendelése, és ha igen, akkor hogyan tudnék Önnel időpontot egyeztetni? (B-A-Z megyéből mennék.)
Előre is köszönöm,
Rita
Az alábbi cím nem az én magánrendelésem. A Budai Allergia Központba jelentkezhet be és ott tudunk konzultálni. Tel: 06-30-631-9309
Jó egészséget kívánok:
A nemrég készült inzulin rezisztencia vizsgálatom eredményével kapcsolatban lenne kérdésem. A 60 perces eredményem 49,50 mIU/L, a 120 perces 50,60 mIU/L, aminél a megadott referenciatartomány 22-79. Eszerint az értékem teljesen jó, az orvosom is ezt mondta, azonban elbizonytalanított, hogy egy meddőségi specialista szerint, akinél tegnap voltam első konzultáción, ez nem megfelelő érték. Ön mit gondol? Válaszát előre is köszönöm.
Nem kívánom sem etikai, sem szakami okokból kommentálni a történteket. Az Ön által leírtak is azt bizonyítják, hogy az egyes laboratóriumi módszerek nagyon eltérőek, ezért a vizsgálatok értékelésében a laboratórium orvosai lehetnek segítségére, akik ezeknek az információknak birtokában vannak, „validálják” az eredményeket, másrészt a hozzáértó endokrinológus, aki megvizusgálja és esetleg célzottan (nem protokoll alapján) kiegészítő vizsgálatokat készít.
Az emberi szervezet sokkal komplikáltabb annál, hogy 1-1 laboratóriumi lelettel meg lehessen válaszolni a problémát."Sok van mi csodálatos, de az embernél nincs semmi csodálatosabb." (Szophoklész)
Jó egészséget kívánok:
Rendszertelen vérzés miatt voltam vérvételen, ahol nézték a pajzsmirigyet.
Eredményem:
TSH 3,29 mikroUI/ML
T4 szabad frakció 1,00 ng/dl
T3 szabad frakció 2,37 pg/ml
Azt szeretném kérdezni, hogy ezen eredmények mutatnak-e valami rosszat? Lehet ebből valamit megtudni, vagy teljesen rendben vannak.
Válaszát előre is köszönöm.
Tisztelettel
Tami
Köszönöm megtisztelő bizalmát. Ön nagyon sok információt leírt, és arra komoly szakvéleményt kért. A kérdései világosak és érthetőek, de a választ etikai és szakmai okokból attól kaphatja meg, aki a korábbi vizsgálatokat végezte. Az egyes laboratóriumi módszerek nagyon eltérőek, ezért a vizsgálatok értékelésében a laboratórium orvosai lehetnek segítségére, akik ezeknek az információknak birtokában vannak, „validálják” az eredményeket. Szakmai véleményt, tanácsot csak úgy tudok felelősen adni, ha nem csak a leírható eredményeket van lehetőségem megítélni, de Önt is láthatom, megvizsgálhatom, és így a klinikai képet, kórtörténetet, labor- és ultrahang eredményeket egyben, egységben holisztikusan értékelhetem. Kérem, hogy keressen fel személyesen, ahol mindent részletesen átnézhetünk, értékelhetünk, a megoldást megtalálhatjuk. A gyorsabb átfutási idő miatt, kérem, hívjon a következő telefonszámon: 0630/631-9309, vagy amennyiben megad egy telefonszámot, felhívjuk időpont-egyeztetés végett. Amennyiben további kérdés merül fel, kérem, forduljon hozzám bizalommal!
Jó egészséget kívánok, tisztelettel:
Nagyon örülök, ha segíthettem.
Tisztelettel:
Sok és fontos kérdést tett fel. Ezek mindegyikére így nem fogok tudni kitérni, de a legfontosabbat igyekszem megválaszolni.Az elmúlt évtized egyik váratlan és nagy jelentőségű biológiai felismerése volt, hogy a psycho-neuro-endokrin- és az immunrendszer nemcsak kölcsönhatásban van egymással, hanem közös biokémiai jeleket használ. Ennek a közös "nyelvnek" a megfejtése a molekuláris biológia és genetika legújabb eredményeinek segítségével vált lehetségessé. Ma még nem ismerjük ennek a sokrétű kölcsönhatásnak minden részletét, azonban jelen ismereteink már elégségek annak kimondására, hogy nem egymástól elkülönült, hanem egy integrált psycho-neuro-endokrin-immunrendszer felelős a szervezet homeosztázisának megőrzéséért . Egyre többet hallunk arról ugynais arról, hogy a stressz is felelős betegségeink kialakulásáért. A munkahelyi feszített tempó, a családi gondok és a pénzügyi nehézségek mind nyomot hagynak a testünkön, és akár a szervezet sav-bázis egyensúlyát is felboríthatják. Mit tehetünk ellene?
Vérünk egy különleges folyadék, mely, ha kimozdul a 7,35 és 7,45 közötti Ph-tartományból, akár meg is hallhatunk. Szervezetünk ezért többszörös védelmi rendszert működtet. A tüdőnk által szállított oxigén, a veséink és a hasnyálmirigyünk is komoly munkát végez ahhoz, hogy ez a kémiai egyensúly ne boruljon fel. Ha ezek a szervek valami miatt másként kezdenek dolgozni, a vér sav-bázis szintje elmozdul. „A savasodás szétmarja a sejteket, szöveteket, apránként belemarja magát a vénába és artériába, mint ahogy nyomot hagy a sav a márványba”. Vigyáznunk kell, mert védelmi rendszereink működését könnyen tönkreteheti az egészségtelen táplálkozás, de a mindennapi komoly feszültség is.
A stressz nem csak egy feszült állapot, ami könnyedén elmúlik, ha kikerülünk egy nehéz helyzetből. „A stressz hosszú távon akár betegség kiindulása is lehet, hiszen azonnal hat a szimpatikus idegrendszerre” .Mindannyian megfigyelhettük már magunkon, hogy egy komolyabb vita után, szaporábban vesszük a levegőt, kiszárad a szánk, erőteljesebben ver a szívünk, másként működik a gyomrunk. Ha mindezt, szinte naponta átéljük, megváltozik testünk működése, és egy idő után képtelen lesz védekezni és megbetegszik. „Felborul az egyensúly és a stressz, mint egy néma gyilkos dolgozni kezd: kialakulnak a szív és érrendszeri betegségek, a daganatok, a pajzsmirigyproblémák és a cukorbetegség”. Jó tudni!A nőket is komolyan érinti a stressz, hiszen ők azok, akik lelkiekben könnyebben sebezhetők. Sokkal erőteljesebben hatnak rájuk a családi és érzelmi konfliktusok. Ezzel szemben a férfiakat elsősorban a munkahelyi és a karrierépítési küzdelmek sodorják stressz helyzetbe.
7 javaslat stressz ellen
1. Ismerjük fel, hogy bajban vagyunk és stresszes életet élünk. Keressük meg a konkrét okot! Tegyük fel magunknak a kérdést: a munkahely, az otthoni légkör, emberi kapcsolatok okozzák a problémát?
2. Ismerjük be, hogy ezen változtatnunk kell. Ha tehetjük, kerüljük el a stresszes helyzeteket és tűzzünk ki új célokat magunk elé.
3. Ha gyökeresen nem tudunk változásokat elérni, próbáljunk meg kevésbé érzelmesen és hevesen reagálni a stresszre. Ne gondolkodjunk visszafelé, ne mondogassuk magunknak „hogy mi lett volna, ha…” Mindig előre tekintsünk.
4. Tanuljuk meg kezelni a stressze adott válaszreakciónkat. Járjunk jógázni, sportolni, keressünk olyan lehetőséget, amivel elsajátíthatjuk a mély légzés- és izomlazítás technikáját. Ismerjük meg a zeneterápia lehetőségeit. Végső esetben használjunk gyógyszeres vagy gyógynövényes feszültségoldást.
5. Változtassunk életmódunkon: szokjunk le a dohányzásról és a kávéról, aludjunk rendszeresen.
6. Próbáljuk meg stabilan tartani az érzelmeinket. Ápoljuk emberi kapcsolatainkat, találkozzunk rendszeresen barátainkkal és rokonainkkal.
7. Törekedjünk arra is, hogy megfelelő önismerettel rendelkezzünk és mindig elérhető célokat tűzzünk ki magunk elé.
Mit tehetünk a stressz okozta savasodás ellen?
Ha sikerül változtatnunk életmódunkon, akkor néhány egyszerű diétás tanácsot is érdemes betartanunk, annak érdekében, hogy testünk könnyebben visszanyerje sav-bázis egyensúlyát. Vacsorára mindig könnyű ételeket együnk. Kerüljük az édes és szénsavas italokat, inkább igyunk, naponta legalább két liter tiszta vizet. Építsünk be étrendünkbe kifejezetten lúgosító hatású ételeket. Burgonya, vaj, nyers tej, tejszín, joghurt, édes- és vöröskáposzta, kelkáposzta, karfiol, paprika, hagyma, petrezselyem, metélőhagyma, gombák, zöldborsó, fehérbab, tök, alma, körte, eper, uborka, fejes saláta, hónapos retek, káposzta, mazsola, ásványvíz, tiszta, természetes növényi olajok kerüljenek a tányérunkra.
Jó tudni!
A stressz olyan információkat juttat az agyba, amik az éhségérzetért felelős központot aktiválják. Ezért a túlterhelt ember szinte folyamatosan eszik, nem érez telítettséget, inzulinszintje állandóan magas, és nagyon gyorsan elhízik. Mindez cukorbetegséghez, vérnyomás problémákhoz, érelmeszesedéshez és pajzsmirigy működési zavarokhoz vezethet.
Stressz teszt
1. Gyakran érzek fáradtságot
2. Próbálok kikapcsolódni, de akkor is a munka jár a fejemben
3. Gyakran elfelejtek dolgokat
4. Reggeli ébredés után is fáradtnak érzem magam
5. Emésztési problémáim vannak
6. Nehezen alszom el, éjszakánként gyakran megébredek
7. Allergiás tüneteim vannak
8. Könnyen ingerlékennyé, dühössé válok
9. Kerülöm mások társaságát, nem járok össze a barátaimmal
10. Egyre gyakrabban kételkedem önmagamban
és abban, hogy helyesen cselekszem
Értékelés
- Ha igen válaszaink száma kevesebb, mint három, viszonylag stresszmentes életet élünk.
- Ha négy vagy öt igen választ adtunk, akkor érdemes elgondolkodnunk azon, mit kellene változtatni az életünkön nyugalmunk és egészségünk érdekében. Vásároljunk gyógyszertárban lakmuszpapírt, amivel megmérhetjük szervezetünk sav-bázis egyensúlya, hogyan reagált a stresszre.
- Öt igen felett viszont mindenképpen keressünk fel egy orvost, aki a segítségünkre lehet.
Jó egészséget kívánok, tisztelettel:
Nagyon köszönöm hogy megtisztelt válaszával és a telefonszámával:
Én vagyok az a 27 nö aki a hirzutismusban szenvedek.
Volna még egy kérdésem önhöz: vizsgálat menyibe kerülne vagy a tb vinanszirozza e nekem a vizsgálatot?
Megtisztelö válaszát elöre is köszönöm Ani
Kérem hívja fel a 06-30-631-9309-es telefonszámot. Ott tudnak további felvilágosítást adni.
Jó egészséget kívánok:
Nemrég kaptam kézhez laboreredményemet, mely szerint az anti-TPO-m 370 IU/mL (ref. <35), a TSH: 2,05 mU/L (ref. 0,4-4), fT4: 11,3 pmol/L (ref.7-15,96). Mire utal, hogy bár a tsh-m és a ft4 eredményeim jónak mondhatók, mégis ennyire magas az anti-TPO? (Addisonom, PCO-m, cukorbetegségem, és hyperprolactinémiám is van ezen kívül.) Volt már két vetélésem, anti-TPO-t akkor nem néztek. Előfordulhat, hogy ez is okozhatta őket?
Ebben az esetben is, hogy a tsh, ft4 jónak mondható, gyógyszeres kezelés várható? Ha igen, akkor az a most normálisnak mondható tsh-t nem fogja rontani?
Bár fT3-at nem néztek most, de amennyiben nem fog - valamilyen kezelés hatására - javulni az anti-TPO-m, érdemes-e rT3-at is nézetni? Ha jól tudom, Mo-on ez nem bevett szokás, azonban annak magas értéke is okozhatja, ha nem javul az anti-TPO értéke.
Válaszát megköszönve,
H.
A rT3-t nem feltétlen kell vizsgálni. A rT3 és az anti-TPO között nincs összefüggés. Az egyes laboratóriumi módszerek nagyon eltérőek, ezért a vizsgálatok értékelésében a laboratórium orvosai lehetnek segítségére, akik ezeknek az információknak birtokában vannak, „validálják” az eredményeket.
Az autoimmun folyamat - miként erre egyik korábbi válaszomban kitértem és az ábrát is mellékletem - megelőzi a hormonális változásokat.
Az autoimmuneredetű pajzsmirigybetegségek (ha kiderül ennek fennállása!), gyakran társulnak más kórképpel. Ezek felhívják a kezelő orvos figyelmét arra, hogy a pajzsmirigybetegség mellett más autoimmun kórkép is jelen lehet. Az egyik, gyakori betegség, a mellékvese gyulladása. Ezt e betegséget Addison kórnak hívja a szakirodalom és előfordulhat önmagában, de a leggyakrabban más betegséghez társul. A csökkent hormontermelése életveszélyes krízist eredményezhet, miként ez az ifjú beteggel is történt. Hasonló betegségben több államférfi (fenti képen J.F. Kennedy) és közismert színész is szenvedett, ill. szenved. Az ún. „kubai válság idején” Kennedy betegsége, amelyet akkor még kevésbé jól tudtak kezelni - majdnem az egész világot háborús válságba sodorta. Kennedy Addison kórját és pajzsmirigy autoimmun gyulladását 1947–ben diagnosztizálták és 36 alkalommal kezelték kórházban.. A kórtörténete alapján Kennedy már ezt megelőzően is szenvedett tünetei alapján ebben a betegségben és az orvosok azt véleményezték, hogy 1 éven belül meghal ebben a betegségben. Végül is – miként azt tudjuk - merénylet áldozata lett 1963-ban.
• Nagyon fontos kitérnem arra, hogy a csökkent mellékvese működés már korábban is fennállhatott, azonban a tiroxin kezelés elkezdése hirtelen váltotta ki a kritikus állapotot. Ezért is lényeges, hogy ne az a séma (protokoll!) működjön, azaz „emelkedett TSH, tehát automatikusan pajzsmirigyhormon kezelés szükséges”, anélkül, hogy a kiváltó okokat és a kísérő betegségeket megvizsgálnák, ill. szükség szerint kezelnénk.
A pajzsmirigy kezelése előtt mindig legyen kérdés az, hogy:
• Van-e mellékvese betegsége, Addison kórja?
• Van-e más immuneredetű endokrin betegsége (pl. inzulinnal kezelt cukorbetegség, mellékpajzsmirigy gyulladás?)
• Van-e más autoimmun eredetű betegsége:
o Meddőség, menzesz zavarok?
o Gyomor-bélgyulladás, nyelvgyulladás?
o Hajhullás?
o Vészes vérszegénység („anaemia perniciosa”)?
o Ízületi gyulladás?
o Vitiligo (bőrfestékhiány)?
o Van-e ismeretlen eredetű alacsony vérnyomás?
o Van-e fokozott hajlam fertőzésekre?
o Van-e idegrendszeri autoimmun betegsége („myastenia gravis, sclerosis multiplex”)?
o Van-e szívizomgyulladása?
Sokszor kérdezik tőlem, hogy társulhatnak-e egymással a fenti kórképek. A válaszom tehát egyértelmű: igen! Ezért az egyik tünet vagy betegség felismerése után az okok keresése mellett arra is gondolni kell, hogy más, társuló betegség van-e, esetleg lappangó formában. Tudom, hogy ez a mechanikussá, „ún. protokollokká” alakult orvoslásban gyakran „elsikkad”, pedig erre gondolni valóban nem pénzkérdés! A kezelésnek is komplexnek, holisztuikusnak kell(ene) lennie.
Jó egészséget kívánok:
Tanácsát szeretném kérni. Az egészségügyi problémáim pár hónappal ezelőtt kezdődtek erős fej és lábfájással, de a fájdalom változó volt. A fejfájást gyakran a tarkómnál éreztem, vagy a homlokomnál volt hogy jobb oldalt, ami pedig a lábamat illeti gyakran bekeményedett a vádlim, feszített a combom és volt hogy a térdem fájt, bizseregtek a lábaim. Reumatológián két alkalommal kaptam szteroid injekciót a fájdalom enyhítésére ami pár napig használt de ezt követően a tünetek visszatértek és mellette még hát és nyakfájdalom is jelentkezett, szédülés, rosszullétek, szemfájdalom / fáradtság illetve alkalmanként szívkörnyéki fájdalom. A tünetek nem egyszerre hanem általában váltakozva jelentkeznek. Egy vérvétel során kiderült hogy a pajzsmirigyem alul működik, a THS érték 5,68 mU/I volt (T4 1.26 , T3 2.90), a kontroll vérképen pedig a TSH 5,59. Az anti TPO érték 489 U/ml amire az orvos azt mondta, hogy nem kell vele foglalkozni. Napi fél Letrox 75 tablettát kezdtem el szedni az elmúlt napokban és 3 hónap múlva lesz a kontrollvizsgálat. Érdeklődni szeretnék hogy mind ezek a tünetek összefüggésben lehetnek e a pajzsmirigy alul működésével valamint interneten olvastuk a professzor úr egy cikkét a szelénhiányról és szeretném megkérdezni hogy ilyen esetben ajánlott e esetleg szelén tabletta szedése.
Válaszát előre is köszönöm
Tisztelettel:
Eszter
Köszönöm megtisztelő bizalmát. A fentiekből nem derül ki a betegségének az oka. A Letrox a csökkent pajzsmirigyműködésre hat, de egyéb hatás nincs.
A szelén hiány fontosabb tünetei:
Csökkent pajzsmirigyműködés (Hypothyroidism )
Csökkent stressztűrő képesség
Hajhullás
Sterilitás különböző formái
Csökkent immunológia védekező képesség
Emelkedett koleszterin szint
Fertőzésekre fokozott hajlam
A bőr korai öregedése
Rosszindulatú betegségekre fokozott hajlam (családi halmozódás)
Szívbetegségek (koszorú érbetegség, ritmuszavarok)
Májkárosodás, májbetegségek
Melyek azok a betegségek, amelyekben ajánlatos a szelén kezelés?
Hypothyroidism ,Pajzsmirigygyulladás
Immunhiányos állapotok
Szívbetegségek
Asthma
Hajhullás egyes formái (autoimmun eredetűek)
Mire és hogyan hat a szelén?
Csökkenti a változó kór tüneteit, a hőhullámokat
Javítja a pajzsmirigy működését, aktiválja a pajzsmirigy hormonjait
Stimulálja az immunrendszert
Biztosítja az egészsége hajat és javítja a bőr rugalmasságát
Méregtelenítő hatású: a dohányzás, az elhízás, az alkohol, egyes gyógyszerek okozta ártalmakat csökkenti
Csökkenti az izületi gyulladásokat
Javítja a máj és a hasnyálmirigy működését
Növeli a libidót, a sexuális „vágyat”, javítja a megtermékenyülés esélyét és fokozza a hím ivarsejtek anyagcseréjét
Képes késleltetni az öregedés folyamatát
Bizonyítottan képes gátolni főleg bizonyos daganatok (pajzsmirigy, prosztata, emlő, máj és hasnyálmirigy)
A szívet és az érrendszert védi, késlelteti az érelmeszesedést , érszűkületben szenvedőkben javítja a keringést, gátolja a fekélyek kialakulását
A szelén ezeket a hatásait sokféle úton fejti ki, a döntő azonban a károsító szabadgyökök elleni védelem.
Figyelmeztetések:
A szelén mérgező is lehet, ha nem megfelelő indikációval és dózisban szedik!!! Clszerű a vérben a szelén szintjének meghatározása és követése.
Jó egészséget kívánok, tisztelettel:
Erős hajhullás miatt kerestem fel a Körzeti orvosomat, régebben is volt már ilyen gondom, akkor nagyon alacsony vas volt a véremben/ 3,9/. Kiderült akkor, hogy refluxom van, a gyomortükrözés pozitív helicobaktert mutatott, a lisztérzékenység negatív lett. A Gasztroenterológusom vérből is csináltatott lisztérzékenységi tesztet, aminek az eredményét még nem tudom. Évek óta puffadási problémáim vannak, az okok még nem derültek ki.Étel és egyéb allergiával is küzködök, naponta antihisztamin tabletát kell szedjek. A jelenlegi laboreredményemen TSH szint 8,34 , az FT4 15,6 . A körzeti orvosom azt mondta, nem írna gyógyszert, de mivel panaszaim vannak, erős hajhullás, fáradékonyság, így szedjem az L-Thyroxint míg eljutok a Pajzsmirigy Ambulanciára. Első 5 napra írt 25 mikrog. , majd 50 mikrog. -ot. Az ultrahang vizsgálaton nem találtak problémát, negatív lett. Átolvasva megannyi írást a pajzsmirigyről, alul és túlműködésről, azt gondolom, nálam nincs nagy probléma, ha más eredményeit és leírásait olvasom. December 5-re kaptam a szakrendelésre időpontot, bejelentkezésnél azt mondták, szedjem nyugodtan addig a gyógyszert, és egy novemberi laboreredménnyel menjek. Kérdésem az lenne, hogy maradhatnék-e a 25 mikrogramm-nál vagy emeljem 50-re, ahogy előirták? A gasztroenterológiai eredményeimet is vigyem az Endokrinológiai szakrendelésre? ..és még egy, lehet \"buta \" kérdés: vérvétel előtti napon spirulina- algaport fogyasztottam, amiben esetleg magas jódtartalom is lehetett. Befolyásolhatta-e a laboreredményemet?
Válaszát megköszönöm!
Tisztelettel: Szikora Andrea
Köszönöm megtisztelő bizalmát. Ön nagyon sok információt leírt, és arra komoly szakvéleményt kért. A kérdései világosak és érthetőek, de a választ etikai és szakmai okokból attól kaphatja meg, aki a korábbi vizsgálatokat végezte. Az egyes laboratóriumi módszerek nagyon eltérőek, ezért a vizsgálatok értékelésében a laboratórium orvosai lehetnek segítségére, akik ezeknek az információknak birtokában vannak, „validálják” az eredményeket. Fontos kiemelnem, hogy nem a laboratóriumi adatokat célszerű kezelni, hanem a beteget. Szakmai véleményt, tanácsot csak úgy tudok felelősen adni, ha nem csak a leírható eredményeket van lehetőségem megítélni, de Önt is láthatom, megvizsgálhatom, és így a klinikai képet, kórtörténetet, labor- és ultrahang eredményeket egyben, egységben holisztikusan értékelhetem. Kérem, hogy keressen fel személyesen, ahol mindent részletesen átnézhetünk, értékelhetünk, a megoldást megtalálhatjuk. A gyorsabb átfutási idő miatt, kérem, hívjon a következő telefonszámon: 0630/631-9309, vagy amennyiben megad egy telefonszámot, felhívjuk időpont-egyeztetés végett. Amennyiben további kérdés merül fel, kérem, forduljon hozzám bizalommal!
Jó egészséget kívánok, tisztelettel:
Köszönöm a válaszát, és a megadott telefonszámot! Sajnos csak januárra tudnának időpontot adni. A nőgyógyász viszont sürgeti a műtétet. Tulajdonképpen a vérzés miatt vennék ki a méhet. Boldog lennék, ha tudna valahogy időd tudna szakítani rám október elején. Október 11-én meg kell jelennem a kórházban a beavatkozás miatt. Mivel évekkel ezelőtt 1 inseminatio után megbolondult a ciklusom, idén szintén felborult a menzeszem és az idén kezdtem szedni a Letroxot. Mikor elkezdtem szedni a gyógyszert rettenetesen hasogatott minden nap a fejem, és a hátamon a bőr száraz és pikkelyes lett, meg elszíneződött, mintha napégette, és koszos lenne. Telefonon egyeztettünk a belgyógyásszal, és kevesebbet kellett szednem akkor jobban lettem.
Biocard celiac test: negatív
Várom válaszát!
Tisztelettel
Nagy Gabriella
Örülök, hogy a Biocard test neg.
Bízom benne, hogy kolléganőm, aki ezen a héten áll majd munkába fog tudni korábbi időpontot adni . A helyzet az, hogy újabb idpontot iktattam be a rendelésre -a szabadságom terhére - , de még így sem egyszerű a dolog. Sajnos a betegek egy része "elfelejt" megjelenni és visszajelezni, amely további gondot okoz.
A csökkentett dózisú Letrox további titrálás és kiegészítése szóbajön.
Jó egészséget kívánok, tisztelettel:
Köszönöm a válaszát, és a megadott telefonszámot! Sajnos csak januárra tudnának időpontot adni. A nőgyógyász viszont sürgeti a műtétet. Tulajdonképpen a vérzés miatt vennék ki a méhet. Boldog lennék, ha tudna valahogy időd tudna szakítani rám október elején. Október 11-én meg kell jelennem a kórházban a beavatkozás miatt. Mivel évekkel ezelőtt 1 inseminatio után megbolondult a ciklusom, idén szintén felborult a menzeszem és az idén kezdtem szedni a Letroxot. Mikor elkezdtem szedni a gyógyszert rettenetesen hasogatott minden nap a fejem, és a hátamon a bőr száraz és pikkelyes lett, meg elszíneződött, mintha napégette, és koszos lenne. Telefonon egyeztettünk a belgyógyásszal, és kevesebbet kellett szednem akkor jobban lettem.
Biocard celiac test: negatív
Várom válaszát!
Tisztelettel
Nagy Gabriella
Örülök, hogy a test negativ. A Letrox bőrszárazságot nem okoz! Amennyiben a csökkentett gyógyszer mellett jobban érzi magát, akkor egyelőre ezt a dózist szedje, de erre a kérdésre feltétlen vissza kell majd műtét után térni, mert az emeltebb dózis megfelelő adagolásssal előnyösebb.
Ui. január előtt lesz majd lehetőség az átszervezés után.
Jó egészséget kivánok:
Égy egy 27 éves nö vagyok és oriási problémával fordulok önhöz.Már gyerek koromban elkezdött nálam ez probléma azt hiszem hivhatom hormonzavarnak evvel elég nehéz együtt élnem .
Kb 9 10 éves lehettem mikor elkezdtem menstruálni és rá 1-2 évre elkezdtem szörösödni mint egy fiu:
A hátamon pattanások voltak és vannak is azota sem mulik el hiába kenyem.
Hát 4 -5 évell ezelött elkeztem hizni pedig figyelek magamra hogy mit eszek már 30kg feleslegem van nagyon fáradékony vagyok ideges és nagyon feledékeny lettem.A belsö combomon pattanás félék jelennek meg hosszukásak néha kmények is és a börön ott kezd elszinezödni.Ha seb vagy egy heg keletkezik rajtam az honapokba keröl mire emulik de a helye lilás feketés marad.Szörösödésem már anyira elfajult hogy borotválkoznom kell és evvel nagyon nehéz együtt élnem sok ember csufolodik rajtam.Még orvosnál nem jártam mert nagyon szégyellem magam hogy ilyen lettem de nem tudom mitöl és nem tudom hogy tudna e rajtam segitei Dr Ur vagy valami gyogy szert felirni hogy ugy élhessek mint a többi nö.Ön az elsö Dr ur akinek leirtam a problémámat kérem segitsen rajtam elöre is köszönöm Ani
A betegséget idegen szóval hirzutizmusnak nevezzük. Ez jelenti azt a kóros állapotot, amikor nőkön fokozott szőrnövekedés jön létre a test azon részein, amelyeken ez a jelenség csak férfiakon szokott előfordulni (bajusz, szakáll, a hasa, mellkas)(1. és 2. ábra).
Ezeket a testrészeket férfihormon-függő, un. „androgén-dependens” régióknak is hívjuk. Ettől a típusú fokozott szőrnövéstől el kell különíteni az un. „hipertrichózis” fogalmát, amely esetben a szőrösödés az egész testre közel egyenletesen kiterjed. Mindkét típusú elváltozás hormonális eredetű, de míg hirzutizmusban a nőkben élettani körülmények között kis mennyiségben is termelődő férfi (androgén) hormonok túlműködése figyelhető meg, a hipertrichózisban más hormonális szervek (pl. pajzsmirigy) kóros működése ludas a tünetek kialakulásáért. A fokozott szőrnövésnek sok oka van. Fontos hangsúlyozni, hogy a jelenséget nem szabad bagatellizálni, mert a látszólag „kisebb” kozmetikai probléma hátterében a hormonális szervek betegségei: gyulladásai, daganatai is állhatnak. A hirzutizmus oka a férfi nemi hormonok fokozott hatása a szőrtüszőkre. Ennek két fő oka lehet:
• A férfi hormonok szintjének emelkedése a vérben
• A hormonok iránti érzékenység fokozódása
A férfi hormonok nőkben a petefészekben és a mellékvesékben (ritkán más szervekben) képződnek. A hormonálisan kevésbé aktív férfihormont, a tesztoszteront, a vérben lévő fehérje, az SHBG („Sex Hormone Binding Globulin”) juttatja el a szervezet különböző részeibe. Az SHBG-ről lehasadó tesztoszteronból a bőrben különböző mennyiségben jelenlévő 5-alfa-reduktáz enzim egy rendkívül aktív férfihormont, a dihidro-tesztoszteront képezi, amely elsődlegesen bűnös a hirzutizmusért.
Milyen gyakori és hogyan állapíthatjuk meg a betegség fennállását?
Az USA-ban a fogamzáskorú nők 10%-át érinti. A genetikai okok fontosságát jelzi, hogy egyes családokban, bizonyos népcsoportokban (mediterrán régiókban élőknél) lényegesen gyakoribb. A betegség diagnosztizálásához a „Ferriman-Gallway” által leírt módszert használjuk. Ennek lényege az, hogy a test 9 különböző részén határozzuk meg a szőrnövekedés mértékét és azt számokban („score”) fejezzük ki (ábra). Az érték (index) kiszámolása endokrinológus feladata. Annyit azonban célszerű tudni, hogy a 8. érték alatt a hirzutizmus enyhe, a 44. érték felett súlyos mértékű.
Milyen betegségek állhatnak a hirzutizmus hátterében?
• PCOS (policisztás ovárium tünet együttes)
• Menstruációs hormonális zavarok
• Mellékvesék túlműködése és daganatai
• Kóros elhízás, fokozott inzulin szint
• Petefészek egyes daganatai
• Pajzsmirigy betegségei
• Egyes gyógyszerek (hidantoin készítmények, egyes hormonális fogamzásgátlók, stb)
Sajnos az esetek többségében nemcsak a hirzutizmus tünetei észlelhetők, hanem paradox módon a fokozott szőrnövés mellett egyes területeken (pl. hajas fejbőrön) a szőrzet ritkulása, kopaszodás is bekövetkezhet!
Az endokrinológus feladata a fenti tünetek megtalálása és kezelése.
Miből állnak a vizsgálatok?
• A személyes találkozás során a tünetek kialakulási idejének, a kórelőzménynek a tisztázása, a korábbi gyyógyszerek, családi adatok felvétele.
• A beteg vizsgálata, a Ferriman-Gallway index kiszámítása.
• Bizonyos hormonális vizsgálatok
• Képalkotó eljárások (CT, MRI szükség estén)
A gyógyulás több tényezőtől függ:
• A beteg korától
• Az alapbetegség természetétől
• A tünetek fennállásának idejétől (az előzetes epilálás rontja a gyógyulás esélyeit!)
Az alábbi típusú gyógyszereket alkalmazhatunk (a betegség természetétől függően):
• Csökkentik a férfihormonok termelődését és vérszintjét
• Növelik a női hormonok mennyiségét és vérben, ill. a bőrben a szintjét
• Gátolják az 5-alfa-reduktáz enzim működését a bőrben
• Befolyásolják a kisiklott pajzsmirigyműködést
Összegezve: a hirzutizmus ma már gyógyítható, de célszerű az okok megkeresése. Az egyes epilálási módszerek egyrészt elfedhetik a bajt, másrészt éppen ellenkező hatást érhetnek el!.
Tel: 06-30-631-9309
Jó egészséget kívánok:
- a teljes kephez le kell irnom,hogy Romaniaban elek, es varosunk kicsit szukolkodik gasztroenterologusokban:)....
Nem tudom merre induljak tovabb, probaljam ujra az endokrinologust, vagy mas jellegu vizsgalatok lennenek celszeruek?.....es ja mar tanacsoltak,hogy menjek pszihiaterhez is (egy idoben kicsit panik beteg voltam, ha utazni kellett fraszt kaptam, mert allando felfazasom volt, es hasmenesem es feltem,hogy nem lesz toalett a kozelben:) ) mert lehet ott a fo gond, de en nem ugy erzem, nem vagyok depresszios, jo a problema megoldo keszsegem, dolgozom, es minden felmeru gondot megoldok, nem kerulom ki oket......
Elore is megkoszonom figyelmet es turelmet, remelem tanacsaival tud majd nekem segiteni a problemam megoldasaban.
Valóban sokrétű tünetegyüttest sorol fel. A leírtak alapján értelemszerűen végleges diagnózist további vizsgálatok nélkül nem adhatok.
Néhány dologra hívom fel a figyelmét:
1. Szénhidrátban, zsírban és kémiai adalékanyagokban gazdag táplálkozásunkkal kedvező feltételeket biztosítunk a gombák elszaporodásához, fő táplálékukat ugyanis ezek a tápanyagok jelentik. A téli időszakban gyakori betegségek kezelése sok esetben antibiotikum segítségével történik. Alkalmazásuk során azonban nem csak a kórokozók pusztulnak el, de a bélrendszerben élő, hasznos baktériumok is. A bélflóra egyensúlyának felborulása pedig szintén a gombák elszaporodásának kedvez.
A tünetek igen szerteágazóak lehetnek: hajhullás, kimerültség, gyakori fejfájás, szédülés, zavarodottság, gyomorfájás, izületi gyulladások, autoimmun betegségek, pajzsmirigy gyulladás, krónikus fáradékonyság szindróma, a menstruáció előtti tünetek, székrekedés, vagy hasmenés, puffadás és az édességek utáni fokozott vágy formájában is jelentkezhetnek.
A Candidiázis kórképének kialakulásában a fentieken kívül számos egyéb, napjainkban különösen jellemző tényező is szerepet játszik. A stresszes életmód, a nem megfelelő táplálkozás, a testmozgás hiánya, fogamzásgátlók szedése, az alkohol, a koffein fogyasztás mind elősegítik a gombák elszaporodását.
A kórokozókkal szemben immunrendszerünk nyújt védelmet. Az immunvédekezésnek több szintje és formája van. Az első védelmi sort a faló fehérvérsejtek (fagociták) képezik, melyek bekebelezik a kórokózókat. Baj az, ha a bekebelezett gombát, ill. egyéb kórokozót a falósejtek nem tudják elpusztítani. A védekezés másik vonalát az un. limfociták (T limfociták) képezik, amelyek megfelelő "tanulás", immunizálódás után képesek a kórokozókat feloldani. A limfociták másik csoportja (B limfociták) olyan ellenanyagokat termelnek, amelyek képesek bevonni a gombát és így elősegítik azok elpusztítását.
Megfelelő védelem hiányában tüneti kezeléssel, gombaölő és a bélflóra egyensúlyát helyreállító szerek alkalmazásával és a megfelelő étrend összeállításával csak átmeneti javulást érhetünk el. Azok esetében azonban, akik folyamatosan visszatérő fertőzésekkel küzdenek mindenképpen ajánlott alaposabb vizsgálatok elvégzése, a háttérben ugyanis a szervezet védekező képességének károsodása állhat. Ilyen esetekben tüneti kezelésekkel csökkenthetők ugyan a panaszok, azonban a fertőzésre való hajlam megmarad, ami a betegség kiújulásához vezet.
Az immunhiányos állapot okozói olyan külső faktorok is lehetnek, mint a krónikus stressz helyezetek, endokrin betegségek (pl. csökkent pajzsmirigy működés), vírusfertőzések, vagy toxikus anyagok (egyes gyógyszerek is). Ezek a szerzett formák megfelelő kivizsgálás után gyógyíthatóak.
2.Lisztérzékenység (cöliakia) és a pajzsmiririgy autoimmun betegség gyakori társulása
A betegség autoimmun eredetű és öröklődő jellegű, amelyet különböző névvel illet a szakirodalom: gyermek- és felnőttkori coeliakia, glutenszenzitív enteropathia, sprue, nem trópusi sprue, idiopathias steatorrhoea, lisztérzékenység.
A betegség lényege: komplex felszívódási zavar (a bél nem képes felszívni a nélkülözhetetlen tápanyagokat), amely többnyire gyermekkorban kezdődik és kezelés nélkül halálhoz vezethet. A betegség kialakulásának oka: gluténnel (a búzafélékben található fehérjével) szembeni érzékenység, amely a bélbolyhok pusztulásához vezet. Az örökletes jelleg mellet szól, hogy a beteg szülőkben lévő gének hordozzák a betegségre való fokozott hajlamot. A legújabb nemzetközi kutatások (Setty M. és munkatársai: Celic disease: risk assessment, diagnosis and monitoring, Mol. Diag.Ther. 2008, 12, 289-98) bizonyították, hogy a szöveti antigének (HLA) II. régiójában található gének: DQ2 vagy a DQ8 felelősek a betegség öröklődéséért . A kóros gének megjelenése azonban nem egyforma. Ez azt jelenti, hogy nem mindenkiben azonos életkorban és súlyossági fokban manifesztálódik a betegség. A sokak által ismert típusos klasszikus tünettriász tagjai a hasmenés, a fogyás és a gyengeség nem mindenkiben egyformán jelennek meg. A klinikai kép többnyire jellegtelenül, fokozatosan, máskor akut bélfertőzés formájában fejlődik ki. Néha enyhék, vissza-visszatérő jellegűek a tünetek, emiatt a betegséget csak későn ismerik fel (vagy "félrekezelik”) A lisztérzékenység sajátosan egy jéghegyhez hasonlítható, amelynek csúcsán találhatók a legsúlyosabb esetek. klinikai tünetek gyermekkorban a szoptatás befejezésével, a gabonafélékkel történő táplálás megkezdése után, 6 és 18 hónapos kor között fejlődnek ki. Étvágytalanság, gyakori, nagy mennyiségű, híg, világos és bűzös széklet, szokatlan apátia és ingerlékenység lehetnek az első tünetek. A has puffadt lesz, a bőr alatti zsírszövet és izomállomány csökken. Folyadék-, elektrolit és fehérjevesztés, kiszáradás, alacsony vércukorszint, ill. kálciumszint, végtaggörcsök majd sokkszerű állapot jöhet létre. Ezt coeliakiás krízisnek nevezzük, amely többnyire halálhoz vezet. Ez a súlyos állapot ritka azóta, hogy felismertük a glutén megvonás gyors és eredményes terápiás hatását. Mindezeken kívül természetesen a felszívódási zavar általános tünetei is jellemzőek, hasonlóan a felnőttekben észleltekkel. A betegség a genetikailag meghatározott „szerv-specifikus” autoimmun kórképek közé sorolható. Az arra hajlamos egyénekben immunológiai folyamat alakul ki, amelynek lényege, hogy antitestek (fehérjék) képződnek a gliadinnal és a szöveti transzglutamináz enzim ellen. A gyulladásos folyamat következménye a bélnyálkahártya károsodása és a súlyos felszívódási folyamattal járó tünetek fellépése (vashiány, fehérjehiány, fogyás, osteoporózis, hormonális zavarok, nyelvgyulladás, szájgyulladás, a végtagokon ödéma, ritkán hasüregi folyadék is kialakulhat). A diagnózis általában nem könnyű a sokszínű tünetek miatt. A genetikai háttér, a kiegészítő, ill. társuló betegségek ismerete, a laboratóriumi vizsgálatok azonban sokat segíthetnek a minél korábbi felismerésben és kezelésben. Korábban a D-xilóz teszt és a bélnyálkahártya szövettani vizsgálata volt szükséges. A legújabb kutatások eredményei a következő fontos megállapításokat tették (Naiyer AJ és munkatársai, Thyroid, 2008, 18, 1171-78), hogy:A transglutamináz II enzim (TGase II) elleni antitestek kimutatása segít a korai felismerésében A korábbi viszonylag időigényes módszer (ELISA) helyett az „immunszenzor vizsgálat meggyorsítja a laboratóriumi teszteket. Ráadásul ezen ígérete módszer alkalmas arra is, hogy az ételekből is kimutatja a nagyon kis mennyiségben jelenlevő glutén fehérjét (Kings College London, UK www.kcl. Ac.uk).Az a felismerés, hogy a pajzsmirigyben is van TGase II fehérje arra utal, hogy a pajzsmirigy autoimmun betegségiben gyakori a tünetszegény, néha tünetmentes lisztérzékenység. Ezt mutatja, hogy az autoimmun pajzsmirigybetegség fő indikátora: az un. TPO elleni antitest és a TGase II fehérje elleni antitestek egyaránt pozitívak ) .A végső következtetés, hogy a lisztérzékenyeknek gondolni kell pajzsmirigybetegségre és fordítva, akik pajzsmirigybetegségben szenvednek, azok között a lisztérzékenység gyakoribb. A csökkent pajzsmirigybetegségben szenvedők gyakran panaszkodnak arról, hogy has puffadásuk van és az alkalmazott a pajzsmirigyhormontól nem fogynak. Ilyenkor a hormon csökkent felszívódásának oka a látszólag tünetmentes coeliakia lehet! Ez lehet atípusos és enyhe forma is, de időben kell gondolni rá.
3.Stressz és savasság
Egyre többet hallunk arról, hogy a stressz is felelős betegségeink kialakulásáért. A munkahelyi feszített tempó, a családi gondok és a pénzügyi nehézségek mind nyomot hagynak a testünkön, és akár a szervezet sav-bázis egyensúlyát is felboríthatják. Mit tehetünk ellene?
Védekezne, ha hagynánk
Vérünk egy különleges folyadék, mely, ha kimozdul a 7,35 és 7,45 közötti Ph-tartományból, akár meg is hallhatunk. Szervezetünk ezért többszörös védelmi rendszert működtet. A tüdőnk által szállított oxigén, a veséink és a hasnyálmirigyünk is komoly munkát végez ahhoz, hogy ez a kémiai egyensúly ne boruljon fel. Ha ezek a szervek valami miatt másként kezdenek dolgozni, a vér sav-bázis szintje elmozdul. „A savasodás szétmarja a sejteket, szöveteket, apránként belemarja magát a vénába és artériába, mint ahogy nyomot hagy a sav a márványba”. Vigyáznunk kell, mert védelmi rendszereink működését könnyen tönkreteheti az egészségtelen táplálkozás, de a mindennapi komoly feszültség is.
Azonnal meglátszik a testen
A stressz nem csak egy feszült állapot, ami könnyedén elmúlik, ha kikerülünk egy nehéz helyzetből. „A stressz hosszú távon akár betegség kiindulása is lehet, hiszen azonnal hat a szimpatikus idegrendszerre” .Mindannyian megfigyelhettük már magunkon, hogy egy komolyabb vita után, szaporábban vesszük a levegőt, kiszárad a szánk, erőteljesebben ver a szívünk, másként működik a gyomrunk. Ha mindezt, szinte naponta átéljük, megváltozik testünk működése, és egy idő után képtelen lesz védekezni és megbetegszik. „Felborul az egyensúly és a stressz, mint egy néma gyilkos dolgozni kezd: kialakulnak a szív és érrendszeri betegségek, a daganatok, a pajzsmirigyproblémák és a cukorbetegség”. Jó tudni!A nőket is komolyan érinti a stressz, hiszen ők azok, akik lelkiekben könnyebben sebezhetők. Sokkal erőteljesebben hatnak rájuk a családi és érzelmi konfliktusok. Ezzel szemben a férfiakat elsősorban a munkahelyi és a karrierépítési küzdelmek sodorják stressz helyzetbe.
7 javaslat stressz ellen
1. Ismerjük fel, hogy bajban vagyunk és stresszes életet élünk. Keressük meg a konkrét okot! Tegyük fel magunknak a kérdést: a munkahely, az otthoni légkör, emberi kapcsolatok okozzák a problémát?
2. Ismerjük be, hogy ezen változtatnunk kell. Ha tehetjük, kerüljük el a stresszes helyzeteket és tűzzünk ki új célokat magunk elé.
3. Ha gyökeresen nem tudunk változásokat elérni, próbáljunk meg kevésbé érzelmesen és hevesen reagálni a stresszre. Ne gondolkodjunk visszafelé, ne mondogassuk magunknak „hogy mi lett volna, ha…” Mindig előre tekintsünk.
4. Tanuljuk meg kezelni a stressze adott válaszreakciónkat. Járjunk jógázni, sportolni, keressünk olyan lehetőséget, amivel elsajátíthatjuk a mély légzés- és izomlazítás technikáját. Ismerjük meg a zeneterápia lehetőségeit. Végső esetben használjunk gyógyszeres vagy gyógynövényes feszültségoldást.
5. Változtassunk életmódunkon: szokjunk le a dohányzásról és a kávéról, aludjunk rendszeresen.
6. Próbáljuk meg stabilan tartani az érzelmeinket. Ápoljuk emberi kapcsolatainkat, találkozzunk rendszeresen barátainkkal és rokonainkkal.
7. Törekedjünk arra is, hogy megfelelő önismerettel rendelkezzünk és mindig elérhető célokat tűzzünk ki magunk elé.
Mit tehetünk a stressz okozta savasodás ellen?
Ha sikerül változtatnunk életmódunkon, akkor néhány egyszerű diétás tanácsot is érdemes betartanunk, annak érdekében, hogy testünk könnyebben visszanyerje sav-bázis egyensúlyát. Vacsorára mindig könnyű ételeket együnk. Kerüljük az édes és szénsavas italokat, inkább igyunk, naponta legalább két liter tiszta vizet. Építsünk be étrendünkbe kifejezetten lúgosító hatású ételeket. Burgonya, vaj, nyers tej, tejszín, joghurt, édes- és vöröskáposzta, kelkáposzta, karfiol, paprika, hagyma, petrezselyem, metélőhagyma, gombák, zöldborsó, fehérbab, tök, alma, körte, eper, uborka, fejes saláta, hónapos retek, káposzta, mazsola, ásványvíz, tiszta, természetes növényi olajok kerüljenek a tányérunkra.
Jó tudni!
A stressz olyan információkat juttat az agyba, amik az éhségérzetért felelős központot aktiválják. Ezért a túlterhelt ember szinte folyamatosan eszik, nem érez telítettséget, inzulinszintje állandóan magas, és nagyon gyorsan elhízik. Mindez cukorbetegséghez, vérnyomás problémákhoz, érelmeszesedéshez és pajzsmirigy működési zavarokhoz vezethet.
Stressz teszt
1. Gyakran érzek fáradtságot
2. Próbálok kikapcsolódni, de akkor is a munka jár a fejemben
3. Gyakran elfelejtek dolgokat
4. Reggeli ébredés után is fáradtnak érzem magam
5. Emésztési problémáim vannak
6. Nehezen alszom el, éjszakánként gyakran megébredek
7. Allergiás tüneteim vannak
8. Könnyen ingerlékennyé, dühössé válok
9. Kerülöm mások társaságát, nem járok össze a barátaimmal
10. Egyre gyakrabban kételkedem önmagamban
és abban, hogy helyesen cselekszem
Értékelés
- Ha igen válaszaink száma kevesebb, mint három, viszonylag stresszmentes életet élünk.
- Ha négy vagy öt igen választ adtunk, akkor érdemes elgondolkodnunk azon, mit kellene változtatni az életünkön nyugalmunk és egészségünk érdekében. Vásároljunk gyógyszertárban lakmuszpapírt, amivel megmérhetjük szervezetünk sav-bázis egyensúlya, hogyan reagált a stresszre.
- Öt igen felett viszont mindenképpen keressünk fel egy orvost, aki a segítségünkre lehet.
További immuno-endokrin kivizsgálást és oki kezelést javaslok:
A koleszterin szintem magas(8,43mmol/l),emiatt kiderült,hogy a TSH:5,27 ,FT4:12,94, ATPO:557.
Nyaki ultrahangos vizsgálaton is voltam, ahol egy 8X4mm -es echodús göböt találtak a jobb oldalamon.
Bal oldalon inhomogén szerkezetű a pajzsmirigy lebenyem.
Letrox nevű gyógyszert kaptam.A göb miatt aggódom,azzal nincs semmi teendő az orvosom szerint.Szerinte jó indulatú.
Miből gondolja? Izotopos kezelés vagy valami mást nem kellene alkalmazni?
Csak ahova én járok ott lehet hogy erre nincs lehetőség.
Ön szerint kellene -e jelen problémáimmal valami más vizsgálatot, vagy kezelést keresnem?
Ön szerint is hanyagolható az a göb?
Köszönettel: egy aggódó beteg
A legújabb, nagy európai populációban végzett vizsgálatok azt mutatták, hogy a pajzsmirigy betegségei népbetegségnek számítanak, mivel a teljes lakosságban a csökkent működés (hypothyreosis) 4,4%-ban, a túlműködés (hyperthyreosis) 1,4%-ban fordul elő. A hypothyreosis a lakosság 0,4%-ban feltűnő formában van jelen és viszonylag könnyű diagnosztizálni a betegek panaszai, a klinikai tünetek és a laboratóriumi leletek alapján. A probléma az, hogy a betegség 4,0%-ban enyhe, nehezebben felismerhető formában mutatkozik és ritkán gondolnak csökkent pajzsmirigy működésre. Ennek egyik jellemző példája, amikor az emelkedett koleszterint szintet kezelik és nem gondolnak arra, hogy ennek hátterében a pajzsmirigy csökkent hormontermelése áll. A USA-ban 16 millió azon egyének száma, akik az emelkedett koleszterin szintjük miatt részesülnek hormonális kezelésben és normalizálódott koleszterin szintjük. A fokozatosan, látszólag minden ok nélkül kialakult csökkent pajzsmirigyműködést korábban „idiopathiásnak” (ismeretlen eredetűnek) tartották. Kiderült, hogy ezeknek a betegségeknek az oka autoimmun folyamat. Nőkben a betegség lényegesen gyakoribb, mint férfiakban (4-5:1).
Az alulműködésnek (hypothyreosis), vagyis a pajzsmirigy alacsonyabb hormontermelésének oka lehet a pajzsmirigy megbetegedése, melynek hátterében állhat gyulladás, a jód hiánya, pajzsmirigyműtét, röntgensugárzás vagy akár gyógyszerek is. Amikor a pajzsmirigyhormon szintje még csak kismértékben tér el a normálistól, a tünetek nem jellegzetesek, így általában nem is tulajdonítunk nekik jelentőséget. Enyhe fáradékonyságon és a koncentrációs képesség romlásán kívül más nem érzékelhető. Komolyabb esetben az anyagcsere lelassul, lassabb lesz a mozgás, a beszéd, a gondolkodás is, érdektelenség alakulhat ki, ami könnyen összetéveszthető a depresszióval. Aluszékonyság, hízás, szorulás, fázékonyság lesz jellemző, az arc felpuffad, a haj ritkává és szárazzá válik, gyakran hullik is, csökkent a libidó (nemi vágy!). Ilyenkor a bőr hideg, száraz, sápadt és durva. A kezek fájhatnak, a körmök töredeznek, a testen ödémák alakulhatnak ki. A pajzsmirigy hormonjainak és az agyalapi mirigy által termelt TSH-nak a meghatározása segít a kórismézésben, de egyetlen hormonérték önmagában nem diagnosztikus értékű! A pajzsmirigy ultrahang vizsgálata fontos vizsgálat, de a betegség pontos diagnózisát önmagában nem biztosítja! A pajzsmirigy alul működése jól kezelhető hormonpótlással és a kísérő, ill. kiváltó betegségek egyidejű gyógyításával. Fontos! A pajzsmirigybetegségekhez gyakorta más tünetek, kórképek is társulnak:.
• Mellékvese csökkent működése
• A szem betegségei. Gyakran allergiásnak gondolt szemtünetek hátterében a Basedow-Graves betegség áll.
• Az idegrendszer általános gyengeséggel járó betegsége (myasthenia gravis) ritkán kerül időben felismerésre, pedig idejében felismerve gyógyítható. Ennek a betegségnek egyik formája a szemen jelentkezik.
• Cukorbetegség: u.n. inzulinhiányos, 1. típusú diabetes mellitus , Magas koleszterin szint!!!
• A bőr festékhiányos betegségei (vitiligo)
• Ismételt vetélés, terméketlenség
Klinikai immun-endokrin vizsgálatot javaslok, amelyben tudok segíteni személyes konzultáció alapján (06-30-631-9309)
Jó egészséget kívánok: